Trigeminal Neuralgia (TN) causes severe pain in the face. It is characterized by sudden, severe, stabbing, or electric shock-like pain, typically on one side of the face (though it can affect both sides in a small percentage of people). The pain episodes can last from seconds to minutes and can be triggered by everyday activities such as talking, chewing, or even touching the face. Drafts can also cause or increase the pain.
The pain can occur in the forehead (4-5%), cheek (30-35%), or jaw (60%) areas. It is common for people with trigeminal neuralgia to seek initial treatments from dentists. Some even have teeth pulled in an attempt to relieve the pain, only to realize later that it did not help control the pain.
Most of the time, trigeminal neuralgia can be successfully managed with medications. Here are the most commonly prescribed drugs for TN:
- Carbamazepine
- Type: Anticonvulsant
- Effectiveness: Considered the first-line treatment for trigeminal neuralgia.
- Mechanism: Stabilizes nerve activity by blocking sodium channels, reducing pain signals.
- Side Effects: Drowsiness, dizziness, nausea, and, in rare cases, serious blood disorders.
- Oxcarbazepine
- Type: Anticonvulsant
- Effectiveness: Similar to carbamazepine, often used when patients cannot tolerate carbamazepine’s side effects.
- Side Effects: Fewer side effects than carbamazepine, but may still include dizziness, fatigue, and nausea.
- Gabapentin (Neurontin)
- Type: Anticonvulsant
- Effectiveness: Sometimes used as an alternative or in combination with other medications, especially when pain is less responsive to carbamazepine.
- Side Effects: Drowsiness, dizziness, and swelling in the extremities.
- Pregabalin (Lyrica)
- Type: Anticonvulsant
- Effectiveness: Similar to gabapentin, often used for nerve pain management.
- Side Effects: Dizziness, weight gain, blurred vision, and dry mouth.
- Baclofen
- Type: Muscle relaxant
- Effectiveness: Sometimes used in combination with anticonvulsants, particularly if muscle spasms accompany the pain.
- Side Effects: Drowsiness, dizziness, and weakness.
- Lamotrigine
- Type: Anticonvulsant
- Effectiveness: Often used when other medications are ineffective or not tolerated.
- Side Effects: Rash, dizziness, and headache.
- Phenytoin
- Type: Anticonvulsant
- Effectiveness: Used when carbamazepine or oxcarbazepine is not effective.
- Side Effects: Nausea, dizziness, and gum overgrowth.
- Clonazepam
- Type: Benzodiazepine
- Effectiveness: Sometimes used for managing pain in combination with other anticonvulsants.
- Side Effects: Sedation, drowsiness, and dependency risk.
- Tricyclic Antidepressants (e.g., Amitriptyline)
- Type: Antidepressant
- Effectiveness: Occasionally used for managing chronic pain in combination with other therapies.
- Side Effects: Drowsiness, dry mouth, and weight gain.
Trigeminal neuralgia has a remitting and relapsing course over time. It may have periodic flare-ups with increased pain severity and frequency. Taking prednisone over a short period of time (1 to 3 weeks) is usually effective in treating these flare-ups.
During remissions, which can last from a few months to several years, medications can be reduced or even stopped. They can be increased or reintroduced should the pain return.
Surgical treatments for trigeminal neuralgia are considered when medications fail to control the pain adequately or cause intolerable side effects. There are several surgical options, depending on the patient’s specific condition, preferences, and health. Here are the most common surgical treatments for trigeminal neuralgia:
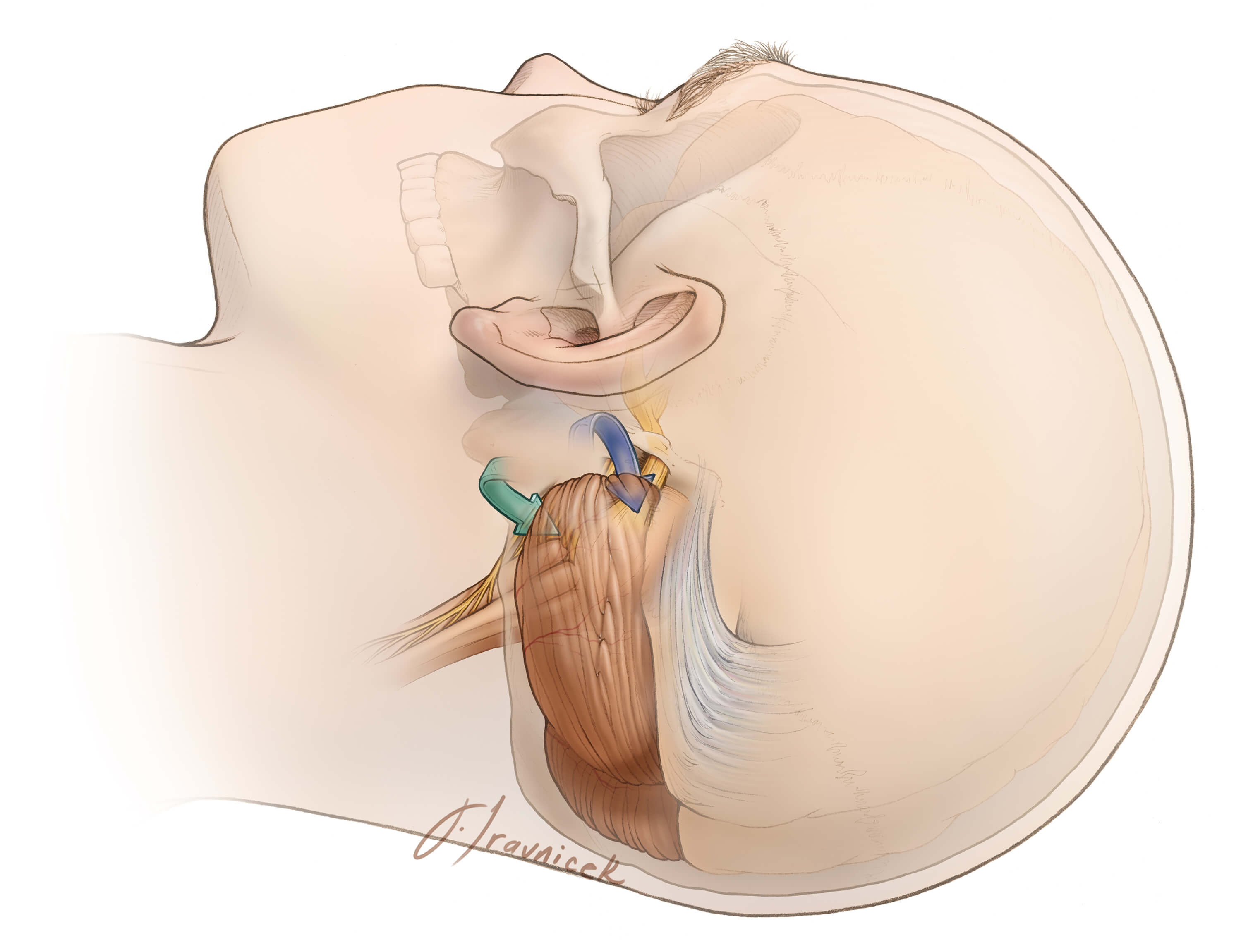
- Microvascular Decompression (MVD)
- Procedure: This is the most effective and long-lasting surgical option. It involves opening the skull and moving or removing any blood vessels that are pressing on the trigeminal nerve, which is usually the cause of the pain.
- Effectiveness: Provides long-term pain relief in most patients.
- Advantages: Preserves nerve function, offering the best chance of pain-free recovery without facial numbness.
- Risks: As with any brain surgery, there are risks of complications, including infection, hearing loss, stroke, or facial numbness. Recovery can take weeks.
- Gamma Knife Radiosurgery (Stereotactic Radiosurgery)
- Procedure: A non-invasive treatment where focused radiation is directed at the trigeminal nerve root to reduce pain. It damages the nerve to block the transmission of pain signals.
- Effectiveness: Can take a few weeks to a few months for pain relief to occur, but it is often successful.
- Advantages: Non-invasive, no incision required, and minimal recovery time.
- Risks: Potential for facial numbness, but lower than with other procedures. Pain recurrence can occur in some patients over time.
- Radiofrequency Rhizotomy (Ablation)
- Procedure: A minimally invasive procedure where a needle is inserted through the cheek to the trigeminal nerve root, and heat (radiofrequency energy) is used to selectively damage the nerve fibers that transmit pain.
- Effectiveness: Often provides good pain relief but is associated with a higher chance of facial numbness compared to MVD.
- Advantages: Can be done under local anesthesia, with quick recovery.
- Risks: Facial numbness is common, and there is a chance that the pain may return over time.
- Balloon Compression
- Procedure: A small balloon is inserted through a catheter into the trigeminal nerve and inflated, compressing the nerve to block pain signals. The balloon is then deflated and removed.
- Effectiveness: Usually provides temporary pain relief and may need to be repeated over time.
- Advantages: Minimally invasive, typically performed under general anesthesia.
- Risks: Risk of facial numbness, but the procedure is generally safe and effective.
- Glycerol Rhizotomy
- Procedure: A needle is inserted through the cheek to the trigeminal nerve, and a small amount of glycerol is injected to damage the nerve and block pain signals.
- Effectiveness: Provides pain relief, but the effect may diminish over time, requiring repeat treatments.
- Advantages: Minimally invasive, with a short recovery period.
- Risks: Some patients experience facial numbness, and the pain may return over time.
- Neurectomy
- Procedure: This involves cutting the affected branches of the trigeminal nerve. It can be done through an open procedure or with a needle.
- Effectiveness: Provides pain relief but results in permanent facial numbness in the area of the nerve that is cut.
- Advantages: Can be effective in certain cases, especially for patients who have not responded to other treatments.
- Risks: Permanent numbness and the potential for recurrence of pain over time.
The choice of surgery should be determined in consultation between the patient, neurologists, neurosurgeons, and radiologists. The availability of a given procedure at the facility can also be a consideration.
Medications can be slowly reduced after surgery if it is successful in controlling the pain. It is common for patients to continue taking some amount of medication after surgical treatments.